This is a blog sharing my personal experience and opinions and is not medical advice or a complete portrayal of the health system in this country
I’m now 9 months into being a doctor and I’ve learnt a lot since my first post – Getting a new name. I’ve also written posts reflecting on my first two rotations as an intern: surgery, and obstetrics, and now it’s time for part 3 – Paediatrics.

This block was one that I had been looking forward to. Paediatricians as a stereotype tend to be absolutely lovely people and thankfully, I found this to be the case when entering the department. That being said, it was also the block that I was a bit worried about. I love kids so what’s the problem? Well, I’m glad you asked, hypothetical reader of this paragraph while I type it alone on my bed. Kids are great, they’re full of life and chaos. I suppose this is part of the reason that it can be so hard to work with sick children, every part of me always seems to say, “this is not how things are meant to be going for you”. A sick child is NOT a happy child.
There’s a large quantity of children that land in hospital in South Africa because of the social circumstances of the country. And I’m really not trying to blame the parents here. I’ve met some dedicated loving parents that are trying their absolute best to care for their child but unfortunately, they just don’t have the knowledge or resources to help. Here’s an article with some stats in it. The block was divided into two parts. Six weeks in the neonatal unit (birth until 1month) and six weeks in the general paeds ward (everyone else up to 12/13 years old).
Neonates

There’s a bit of a joke that when you see a healthy baby after working with sick babies, they just look massive. I’ve gone to review a baby in the maternity ward and been surprised that this was a 1 day old child. It’s difficult not to compare them to the 60 day old baby in the high care nursery that still hadn’t reached that size. If you followed along on my daily reflections on Instagram, you may recall that I have a newfound love of babies crying. I know how that sounds, really. But, after standing next to the open incubator in theater at 2am while waiting for the obstetrics team to cut a lady open because the baby’s heartbeat had started dipping, the sound of a baby being most indignant at being removed from their comfortable hotel with temperature control and on demand food supply into a space filled with cool air, loud noises and strange sensations is a sound that calms my sprinting heart (and I know what my heart rate was while waiting because the easiest way to test the sats monitor is on yourself).
Knowing that there are people that you can call on to help in those times when you aren’t lucky enough to hear an immediate scream is a great relief. You just have to keep going for those minutes until they arrive (v e r y s l o w m i n u t e s). I’d breathe a bit easier when certain anaethetists (who had worked in paeds recently) were on call, the midwife was an experienced one, or I knew my MO was on the same floor of the hospital at that moment. Throughout my three months I was incredibly fortunate to only have one time when a full resus of CPR, adrenaline, and intubation was immediately needed. There were many tiny babies who needed a little extra help breathing but most of them seemed to have the heart-beating part of life sorted.
Paediatrics

There’s a lot more maths involved in paediatrics than in most other departments. Each medication needs to be worked out per the weight of the child. My phone’s calculator became my best friend. I used to be quite good at maths and mentally working out problems. However, it’s just not worth trusting my mental maths when there’s a possibility of giving a toxic dose to a child (shout out to the pharmacists for all their hard work in catching our mistakes). So when you see a doctor staring at their phone, it isn’t social media that has them so entranced but rather they’re likely looking up some piece of information rather than trusting their fallible mind at 2am. Except, it’s also entirely likely that they’re checking whatsapp, not to message friends but because it would appear that most of the South African health care system communication is held together by departmental whatsapp groups (but if it’s me, instagram is also a real possibility). One is far more likely to be distracted from one’s work by the kids running around the ward demanding you make them a paper aeroplane or look at their picture or pick them up or listen to their story.
While most children in hospital are feeling very sorry for themselves and lying in bed, there are those who are sick but do not feel that way or don’t have adequate home situations to care for their conditions and so wait in hospital until a bed opens up at a step-down facility. There were a few children in the ward that were there before I was and are still there after I have moved on to my next rotation. These kids are often incredibly bored as they don’t have access to school or volunteers because of covid. It wasn’t an uncommon sight to see the doctors ward round involving some younger participants as we all traipsed by each patient one by one.

Tuberculosis was one of the worst offenders in long term hospitilisations. It’s a disease with which every South African doctor becomes intimately familiar. An illness that is on almost every differential diagnosis for anyone presenting to hospital, no matter what their symptoms. The other far too common condition is severe acute malnutrition. It’s nowhere near as common as TB but the fact that it exists at all in a world where there should be enough food for everyone makes my eyelids twitch. Parents try their best but guidelines on formula are there for a reason. The milk should not be diluted more to make the preciously expensive can of powder last a little longer. Rooibos tea with all its many benefits cannot be the primary diet of a child. There’s just not enough nutrients in it to feed a growing human.
Covid

Then as much as it isn’t a part of paeds, there was one big other component to my third block. The third wave. The co-vee-dee, the panini, the ‘Uncle Cyril grounded us again’. While there were always meant to be six interns (five when one was on leave) in the rotation at any one time the reality was a little different. On a few days we had 1 post call, 1 on leave, 1 sick with covid, and 1 working in the covid ward, which left 1 in the neonatal ward and 1 in the paeds ward (and if it was paeds turn to cover covid icu that night, it meant the medical officer would be doing the night portion of the 24hr call alone). So when healthcare workers say they have to work twice as hard during a wave, it’s literal. You needed to be doing the work of two or three.
There’s a lot to say about covid and so while I get around to writing this in the trough between the peaks, I can’t help but reflect on what an absurd situation it is. At the time, one must just push through, it’s only once one gets back to something resembling the status quo that one realises how mind-numbingly awful it was.
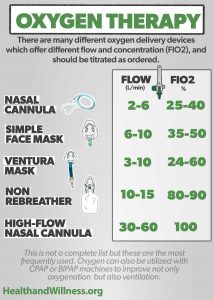
The harsh reality is that there isn’t a whole lot you can do for a patient with severe covid pneumonia other than give them oxygen (this is a vastly simplified statement but that’s how it feels). Once a patient is admitted to the covid ward they make it onto one of 5 oxygen options. Nasal prongs deliver oxygen at flows between 1 and 5 liters per minute giving you 25-40% oxygen instead of the room air oxygen of 21%. Venturi masks between 5-10 liters at 25-60% and non-rebreathers/polymasks at 10-15l per minute with oxygen of 80-90%. After that, we combine the polymask and nasal prongs to “double barrel” it. This does however then use two oxygen ports. If you’re needing more than that then you need high flow nasal cannula that can give 20-60l/min of 100% oxygen. If you’re still struggling to maintain your body oxygen levels (oxygen saturation/sats) then a poly mask is sometimes added over the high flow. The only next option available is intubation and ventilation. The person is sedated and paralysed and a machine takes over the breathing (also on 100% oxygen).
By the time high flow or intubation is required, the person needs to be in a high care or icu setting (I say high care or icu but actually icu is needed, the reality being that during a wave there’s not enough qualified staff to count the set up as an icu). In order to staff the newly set up covid icu, interns were expected to do night shifts in there (thankfully with a more senior doctor as well). This meant you cared for all the patients in the high care/icu, admitted any new covid patients to the ward and were the one called for any resus or death certification. During my shifts, we averaged two deaths a night in an 18 bed unit. This was the most common way for beds to open up and become available for new admissions. There were criteria for whether a person qualified for high flow oxygen or intubation. The older you were, the more comorbidities, the worse your blood results (organ dysfunction markers); the lower your priority score and the more likely your highest intervention level was going to be double barreled oxygen in the general ward.
So although paeds got a little hijacked by covid, my enjoyment of the block was immense and my memories dear. There’s many more things that I want to talk about from this time but I think I’ll leave it at that. Dear reader of this random spew of thoughts, you are always welcome to reach out to me with questions or comments or experiences of your own.

2 comments